Gout is an inflammatory form of arthritis driven by excess uric acid (urate) in the body. When urate levels stay high for long enough, needle-like monosodium urate crystals can form in and around joints. The immune system reacts strongly to these crystals, producing sudden pain, swelling, warmth, and redness, often starting in the big toe but also affecting ankles, knees, feet, wrists, and fingers.
While many people have elevated urate without symptoms, gout becomes more likely when urate rises above the blood’s ability to keep it dissolved. The causes and risk factors below explain why urate climbs and why some people develop painful flares while others do not.
What Actually Causes Gout?
Gout happens when hyperuricemia (high blood urate) leads to crystal formation and inflammation. Uric acid is created when the body breaks down purines, natural substances found in human cells and many foods. Normally, urate dissolves in blood, travels to the kidneys, and leaves the body through urine.
Problems begin when the body produces too much urate, excretes too little, or both. Most cases involve reduced kidney excretion, meaning urate builds up even if production is not extremely high. Crystal formation is encouraged by factors like cooler joint temperatures, dehydration, sudden shifts in urate, and local joint stress.
Core Mechanisms That Raise Uric Acid
1) Reduced Uric Acid Excretion (Most Common)
The kidneys remove a large share of urate each day, and small changes in kidney handling can raise blood levels. Chronic kidney disease (CKD), dehydration, and certain medicines reduce urate clearance. Even mild kidney inefficiency can slowly push urate upward over time.
This mechanism is especially important because it explains gout in people who do not consume high-purine diets. If urate cannot leave efficiently, the blood level stays elevated and crystals can accumulate. Over years, this can also promote tophi (urate deposits under the skin) and kidney stones.
2) Increased Uric Acid Production
Some people produce more urate due to higher purine turnover. Rapid cell breakdown increases purines, which become urate during metabolism. This can occur in conditions with high cell turnover or during treatments that break down cells quickly.
Diet can also increase production, especially when intake includes frequent organ meats, certain seafood, and heavy alcohol use. Production-related hyperuricemia is less common than under-excretion, but it can sharply worsen gout risk when paired with reduced kidney clearance.
3) Inflammation Triggered by Crystal “Shedding”
A gout flare is not just high urate; it is an immune reaction to crystals. Flares often follow sudden changes in urate levels, which can cause crystals to shift within the joint. Triggers include alcohol binges, dehydration, fasting, acute illness, surgery, and starting or stopping certain medications.
Even a minor injury or unusual joint stress can help trigger inflammation in a crystal-prone joint. Over time, untreated hyperuricemia increases the size and number of deposits, making flares more frequent. The long-term driver remains persistent elevated urate.
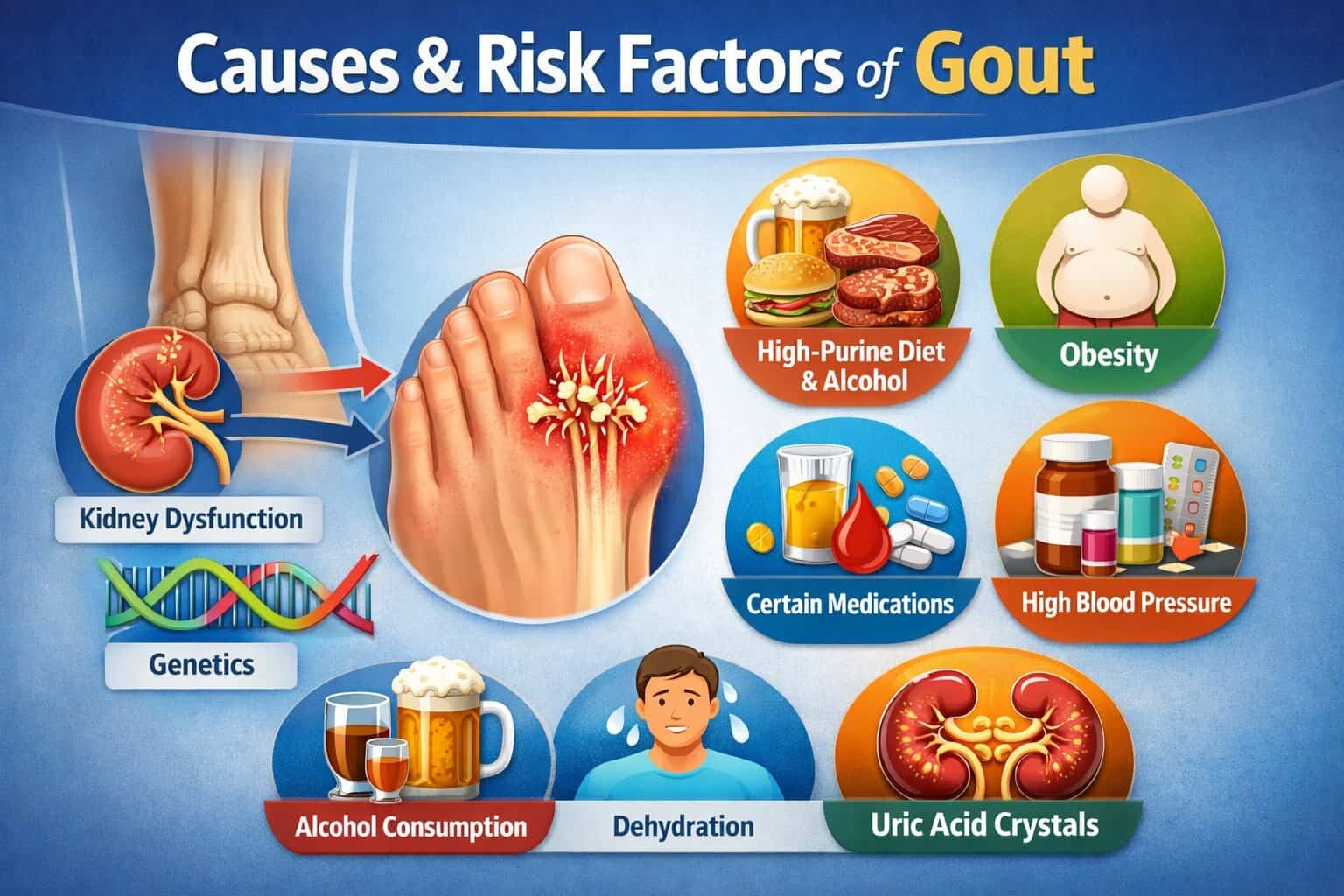
Major Risk Factors for Gout
Genetics and Family History
Genetics strongly influences urate levels through kidney transport proteins. People with a close relative who has gout are more likely to develop hyperuricemia. Some genetic variants reduce the kidney’s ability to excrete urate, raising lifetime risk.
Family history does not guarantee gout, but it shifts the baseline risk higher. When genetic susceptibility combines with lifestyle factors like alcohol intake or weight gain, urate can rise faster. This is one reason gout may appear earlier in some families.
Sex, Age, and Hormones
Gout is more common in men, especially in middle age. In women, risk rises after menopause because estrogen supports urate excretion. As estrogen levels decline, urate levels often climb, increasing gout likelihood later in life.
Age also matters because kidney function and metabolic health often change over time. Years of mildly elevated urate can eventually lead to crystal deposits. Longer exposure increases the chance of flares and chronic gout complications.
Excess Body Weight and Central Obesity
Higher body fat, especially abdominal fat, is linked to higher urate production and reduced excretion. Obesity often overlaps with insulin resistance, which affects kidney urate handling. This combination increases the chance of persistent hyperuricemia.
Weight gain can also raise inflammation markers and stress weight-bearing joints. Mechanical stress may not cause gout alone, but it can contribute to where flares appear. Reducing excess weight often lowers urate and flare frequency.
Diet Patterns That Elevate Uric Acid
Diet does not explain every case, but certain patterns raise risk significantly. High intake of organ meats, red meat, and purine-rich seafood can raise urate production. Frequent consumption increases the average urate load the body must eliminate.
Sugary drinks and foods high in fructose are also important because fructose metabolism can increase urate. This effect is distinct from purines and can be strong when fructose intake is high. Diet matters most when combined with other risk factors like kidney issues or alcohol use.
Alcohol Use, Especially Beer and Spirits
Alcohol increases urate through multiple pathways, including reduced excretion and increased production. Beer is particularly associated with gout because it contains purines from yeast along with alcohol. Heavy drinking patterns raise urate and can trigger acute flares.
Binge drinking can also lead to dehydration and sudden urate shifts, which promotes flare onset. Even in people on urate-lowering therapy, alcohol binges can provoke attacks. Consistency and moderation matter more than occasional small exposures.
Kidney Disease and Reduced Kidney Function
Because the kidneys are central to urate removal, any decrease in function raises gout risk. CKD can make urate remain elevated even with careful diet. Kidney-related hyperuricemia often leads to more persistent elevations and a higher chance of chronic gout.
Kidney stones are also related, especially uric acid stones. Stones can be both a result of high urate and a clue that urate levels have been high for a long time. Monitoring kidney health is crucial in gout prevention and control.
High Blood Pressure and Metabolic Syndrome
Hypertension and metabolic syndrome are strongly linked with hyperuricemia. Insulin resistance reduces the kidney’s urate excretion, increasing blood levels. The cluster of abdominal obesity, high triglycerides, low HDL, and elevated glucose increases gout risk.
This connection explains why gout often appears alongside cardiovascular risk. The conditions share metabolic drivers, and some treatments can also influence urate. Addressing the overall metabolic pattern helps reduce long-term gout burden.
Diabetes and Elevated Blood Sugar
Type 2 diabetes and insulin resistance are associated with impaired urate clearance. High blood sugar may also correlate with dietary patterns that increase urate, such as higher fructose intake. The overlap with obesity and hypertension strengthens the association.
While diabetes does not guarantee gout, it increases the probability of sustained hyperuricemia. Better metabolic control often improves urate handling indirectly. Treating insulin resistance can support a more favorable urate balance.
Medication-Related Risk Factors
Some medications raise urate by reducing kidney excretion. This does not mean they are unsafe, but people at risk may need monitoring.
Common medication categories linked to higher urate include:
- Thiazide diuretics and loop diuretics (often used for blood pressure or fluid retention)
- Low-dose aspirin (can reduce urate excretion in some people)
- Cyclosporine and some other immunosuppressants
- Certain anti-tuberculosis medicines (e.g., pyrazinamide)
Medication effects vary by dose and individual risk. When urate rises after starting a drug, it may reveal an underlying tendency toward gout. Adjustments should be guided by a clinician, especially for blood pressure and transplant-related drugs.
Health Conditions That Increase Uric Acid Production
Some illnesses increase purine breakdown, leading to more urate formation. These conditions can cause significant hyperuricemia, sometimes rapidly.
Examples include:
- Blood cancers such as leukemia and lymphoma
- Psoriasis with high skin cell turnover
- Treatments causing rapid cell destruction (e.g., some chemotherapies)
- Severe hemolysis or tissue breakdown after major illness
In these settings, urate can rise quickly and may require proactive management. The risk is often higher when kidney function is reduced or hydration is inadequate. Preventive strategies are commonly used during high-risk treatments.
Trigger Factors That Precipitate Gout Flares
A flare is often triggered by a short-term stressor acting on a joint already exposed to high urate. These triggers do not always raise urate dramatically; they can shift crystal balance.
Common flare triggers include:
- Dehydration from heat, illness, or low fluid intake
- Alcohol binges, especially beer
- Heavy meals rich in purines
- Fasting, crash dieting, or rapid weight loss
- Surgery, trauma, or acute infections
- Sudden changes in urate from starting, stopping, or altering certain medications
These triggers are important because people may have long symptom-free periods until a stressor activates inflammation. Avoiding triggers can reduce flare frequency but does not replace managing the underlying hyperuricemia. Long-term control focuses on keeping urate consistently lower.
Table: Key Causes vs. Risk Factors
| Category | What It Means | How It Raises Gout Risk |
|---|---|---|
| Under-excretion | Kidneys remove less urate | Most common driver of hyperuricemia |
| Overproduction | Body makes more urate | Higher urate load from purines/cell turnover |
| Genetics | Inherited urate-handling traits | Higher baseline urate and earlier onset |
| Obesity / insulin resistance | Metabolic changes affect kidneys | Less urate excretion + more production |
| Diet (purines, fructose) | High-risk intake patterns | Increased urate formation and flare triggers |
| Alcohol | Multiple metabolic effects | Reduced excretion + dehydration risk |
| Kidney disease | Lower filtration and secretion | Persistent hyperuricemia, stones, chronic gout |
| Medications | Drug-related urate changes | Reduced urate clearance in susceptible people |
Table: Food and Drink Patterns Linked to Higher Gout Risk
| Pattern | Examples | Why It Matters |
|---|---|---|
| High-purine meats | Organ meats, frequent red meat | More purines converted to urate |
| Certain seafood | Anchovies, sardines, shellfish | Higher purines in repeated servings |
| Fructose-heavy drinks | Sodas, sweetened juices | Fructose metabolism can increase urate |
| Alcohol (beer, spirits) | Beer, liquor binges | Reduced excretion + dehydration + purine content (beer) |
| Low hydration | Minimal water intake | Concentrates urine and reduces urate elimination |
Who Is at Highest Risk?
Risk increases when multiple factors overlap. A person with mild kidney impairment, central obesity, and regular alcohol intake has a higher chance of sustained hyperuricemia. Family history further raises the baseline, meaning gout can appear with fewer lifestyle triggers.
People with hypertension or metabolic syndrome are also commonly affected because of shared metabolic pathways. Certain medications can amplify risk in those already predisposed. The most consistent predictor remains persistently elevated serum urate over time.
Practical Takeaways
Gout is caused by urate crystal deposition after long-term hyperuricemia. The most common underlying driver is reduced kidney excretion, often worsened by metabolic factors. Diet and alcohol can raise urate and act as powerful flare triggers, especially in genetically susceptible individuals.
The strongest risk clusters include male sex, post-menopause in women, obesity, kidney disease, hypertension, and alcohol use. Medication effects and high cell-turnover conditions can also push urate high enough to cause gout. Reducing risk depends on identifying which drivers apply and targeting the factors that keep urate elevated.