Gout is a crystal-induced inflammatory arthritis caused by elevated serum urate that leads to monosodium urate (MSU) crystal formation. These crystals can deposit in joints, soft tissues, bursae, tendons, and the kidneys. The “type” of gout describes how the disease behaves over time, from sudden flare-ups to persistent inflammation and visible deposits.
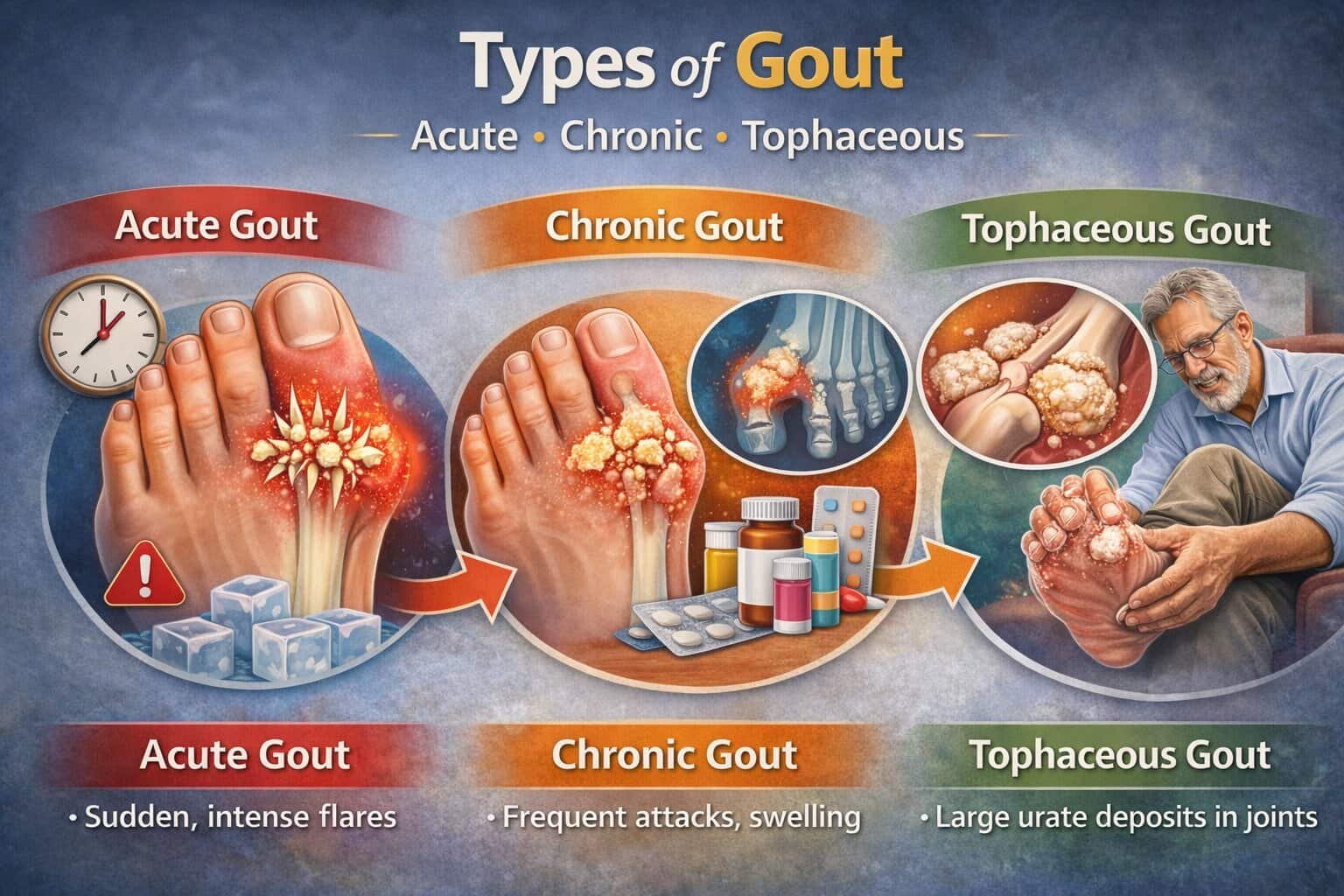
Clinically, gout is most often discussed in three major forms: Acute gout, Chronic gout, and Tophaceous gout. Each represents a different pattern of symptoms, tissue involvement, and long-term risk. Understanding the differences helps guide treatment intensity, monitoring, and prevention of complications.
Quick Overview: How the Types Differ
Acute gout is defined by sudden, severe flares with symptom-free periods in between.
Chronic gout develops when urate stays elevated for years, leading to frequent attacks and persistent joint inflammation.
Tophaceous gout is an advanced form where tophi (urate deposits) form as firm nodules in tissues, often with joint damage and functional limits.
These forms are not separate diseases. They are different expressions of the same urate-driven process, usually progressing when urate remains above the level where crystals dissolve.
Table: Core Differences Between Acute, Chronic, and Tophaceous Gout
| Feature | Acute Gout | Chronic Gout | Tophaceous Gout |
|---|---|---|---|
| Pattern | Sudden flares with full recovery between | Frequent flares + persistent inflammation | Chronic disease + visible urate deposits |
| Pain intensity | Often very high at onset | Moderate-to-severe, recurrent | Variable; pain from inflammation + structural damage |
| Joint involvement | Often one joint at a time early | Multiple joints over time | Multiple joints + tendons/bursae |
| Symptom-free intervals | Common | Short or absent | Often absent |
| Structural damage | Minimal early | Increasing risk | High risk of erosions and deformity |
| Key hallmark | Rapid flare, dramatic inflammation | Ongoing synovitis and attacks | Tophi, erosive changes, disability risk |
The Natural Course of Gout: Where “Types” Fit
Gout often follows a predictable timeline:
- Asymptomatic hyperuricemia: high urate with no symptoms.
- Acute gout flares: intermittent attacks with normal feeling between episodes.
- Intercritical gout: the symptom-free phase between flares, when crystals may still be present.
- Chronic gout: frequent attacks and ongoing inflammation due to continued crystal burden.
- Tophaceous gout: advanced stage with tophi and joint/tissue damage.
Progression is not inevitable. Keeping urate consistently low reduces crystal load and can prevent chronic and tophaceous disease.
1) Acute Gout
What Acute Gout Means
Acute gout is a sudden inflammatory flare triggered when MSU crystals provoke a strong immune response. The onset is typically rapid, building to peak pain within hours. The involved joint becomes hot, swollen, red, and extremely tender, often making even light contact intolerable.
Early disease commonly affects a single joint, classically the first metatarsophalangeal joint (big toe), a pattern called podagra. Ankles, knees, midfoot, wrists, and elbows are also common targets.
Typical Symptoms and Pattern
Acute gout flares often show consistent features:
- Abrupt onset, frequently at night or early morning
- Severe pain with marked swelling and warmth
- Shiny, red skin over the joint
- Limited range of motion due to pain and effusion
- Possible low-grade fever and fatigue in intense attacks
Without effective anti-inflammatory treatment, many flares subside over days to weeks. Afterward, symptoms can fully resolve, which can mislead patients into thinking the condition has “gone away.”
Common Triggers for Acute Flares
Flares are often precipitated by rapid shifts in urate balance or local stress:
- Dehydration, heat exposure, or low fluid intake
- Alcohol, especially binge patterns and beer
- Heavy meals rich in purines or fructose
- Acute illness, surgery, trauma, or intense exertion
- Rapid weight loss, fasting, or crash dieting
- Starting or stopping certain medications that affect urate
Triggers do not create gout by themselves. They typically activate inflammation in a joint that already contains crystal deposits.
How Acute Gout Is Confirmed
The strongest confirmation is joint aspiration showing MSU crystals under polarized microscopy. Clinically, acute gout can resemble infection, and confirming the diagnosis matters because the wrong treatment can delay care.
Useful diagnostic elements include:
- Serum urate (may be normal during a flare, so timing matters)
- Inflammatory markers (often elevated but not specific)
- Imaging when aspiration is not possible: ultrasound signs like the double contour sign, or dual-energy CT identifying urate deposits
Management Priorities in Acute Gout
Acute gout treatment focuses on rapid inflammation control and pain relief:
- NSAIDs at effective anti-inflammatory doses (when appropriate)
- Colchicine early in the flare to reduce inflammatory signaling
- Corticosteroids (oral, intramuscular, or intra-articular) when NSAIDs/colchicine are not suitable
- Rest, ice, elevation, and hydration to reduce local stress
The goal is to shorten the flare and restore function while also planning long-term urate control if flares recur.
2) Chronic Gout
What Chronic Gout Means
Chronic gout occurs when urate remains high for years, leaving a large crystal burden in tissues. Instead of isolated episodes, patients develop recurrent flares, persistent low-grade inflammation, and progressive joint injury. The disease becomes less “on/off” and more continuously active.
Chronic gout often reflects insufficient long-term urate management or delayed diagnosis. It is associated with more comorbidities such as kidney disease, hypertension, metabolic syndrome, and diabetes, which can also complicate treatment choices.
Clinical Features of Chronic Gout
Chronic gout has a distinct pattern:
- Flares become more frequent and may overlap
- Pain can persist between attacks due to ongoing synovitis
- Multiple joints become involved over time
- Stiffness and reduced mobility increase, especially in feet and ankles
- Inflammation may extend to bursae and tendons, causing swelling beyond the joint line
Chronic gout can be mistaken for other inflammatory arthritides because the presentation becomes less dramatic and more persistent.
What Happens Inside the Joint
With ongoing hyperuricemia, crystals continue to deposit, driving repeated immune activation. Over time, this results in:
- Synovial thickening and chronic inflammation
- Cartilage wear and altered joint mechanics
- Bone erosions driven by inflammatory pathways around crystal deposits
- Increased sensitivity to small triggers
Chronic inflammation also contributes to reduced muscle strength and decreased activity, which can worsen metabolic risk factors.
Diagnosis and Monitoring in Chronic Gout
Monitoring becomes central in chronic disease because symptoms alone no longer reflect crystal burden. Key components include:
- Serial serum urate measurements to confirm sustained control
- Assessment of flare frequency, joint function, and physical limitations
- Imaging for structural damage: X-ray for erosions, ultrasound for crystal burden, and DECT where available
- Screening for kidney involvement and uric acid stones if suspected
Management Priorities in Chronic Gout
Chronic gout requires two parallel strategies:
- Lower urate long-term to dissolve crystals and prevent future deposition
- Control inflammation during the period when crystals are being mobilized and flares can occur
Core elements include:
- Urate-lowering therapy (ULT) with treat-to-target dosing
- Anti-inflammatory prophylaxis when initiating or escalating ULT
- Addressing contributing factors: weight, alcohol, diet patterns, hydration, and medication review
Sustained urate reduction is what changes the trajectory of chronic gout. Without it, symptom control alone often fails as crystal deposits accumulate.
3) Tophaceous Gout
What Tophaceous Gout Means
Tophaceous gout is an advanced form characterized by tophi, which are firm nodular deposits of MSU crystals surrounded by chronic inflammation. Tophi most often develop after years of uncontrolled urate levels, though they can appear earlier in severe hyperuricemia or in patients with reduced urate excretion.
Tophi are more than cosmetic findings. They signal a large crystal burden and are associated with erosive joint damage, tendon problems, and disability.
Where Tophi Commonly Appear
Tophi can form in many locations, especially cooler peripheral tissues:
- Helix of the ear
- Fingers and toes, especially near joints
- Olecranon bursa (elbow)
- Achilles tendon and other tendons
- Prepatellar bursa (knee)
- Around the big toe joint and midfoot
- Less commonly, deeper tissues and internal sites
Tophi may be painless at first but can become tender, inflamed, or ulcerate. In some cases, chalky material may drain if the overlying skin breaks down.
Complications of Tophaceous Gout
Tophaceous gout can lead to significant morbidity, including:
- Joint deformity and chronic pain from erosions and cartilage loss
- Reduced range of motion due to mechanical obstruction by deposits
- Tendon thickening and risk of tendon rupture, particularly the Achilles
- Nerve compression syndromes when deposits form near nerve pathways
- Skin ulceration or secondary infection over prominent tophi
- Increased risk of kidney stones and chronic kidney function decline in some patients
Because tophi represent established crystal masses, they usually require more aggressive urate lowering and longer time to resolve.
How Tophaceous Gout Is Diagnosed
Diagnosis is often clinical when classic tophi are visible. Confirmation can be obtained by:
- Aspirating a tophus and identifying MSU crystals
- Imaging: ultrasound can show heterogeneous deposits; DECT can map urate; X-ray can show characteristic punched-out erosions with overhanging edges
Tophi may be mistaken for rheumatoid nodules or other soft-tissue masses, so crystal confirmation is valuable when presentation is atypical.
Management Priorities in Tophaceous Gout
Tophaceous gout requires sustained, targeted urate reduction to gradually dissolve deposits. Effective care typically includes:
- Treat-to-target ULT with careful titration until urate stays consistently below goal
- Prophylaxis against flares during ULT escalation
- Monitoring to document shrinking tophi and improved function
- Consideration of procedural or surgical approaches when tophi cause mechanical impairment, ulceration, or nerve compression
Tophi can shrink substantially when urate is controlled long-term, but regression often takes months to years depending on deposit size and prior disease duration.
Table: Typical Joint Distribution by Gout Type
| Body area | Acute gout common? | Chronic gout common? | Tophaceous gout common? |
|---|---|---|---|
| Big toe joint | Yes | Yes | Yes |
| Ankle / midfoot | Yes | Yes | Yes |
| Knee | Yes | Yes | Yes |
| Wrist / fingers | Sometimes | Yes | Very common |
| Elbow / olecranon bursa | Sometimes | Yes | Very common |
| Achilles tendon | Sometimes | Yes | Very common |
| Ear helix | No | No | Classic site |
Acute vs Chronic vs Tophaceous: Key Clinical Clues
Clues Suggesting Acute Gout
- Single joint, dramatic onset, severe pain within hours
- Redness and warmth that look disproportionate
- Complete resolution between episodes early in the course
Clues Suggesting Chronic Gout
- Increasing flare frequency with incomplete recovery
- Multiple joints involved, persistent swelling or stiffness
- Ongoing tenderness and functional decline
Clues Suggesting Tophaceous Gout
- Firm nodules at typical sites (ears, elbows, fingers, toes)
- Visible deformity, reduced motion, chronic pain
- Imaging evidence of erosions and urate deposits
Why “Intercritical” Periods Matter
Between acute flares, many patients feel normal, but crystals often remain. This intercritical phase can include silent inflammation and ongoing deposition if urate remains elevated. Over time, crystal burden increases and makes chronic disease more likely.
This is why long-term urate control is central even when attacks are infrequent. The absence of pain does not necessarily mean the absence of disease activity.
Differential Diagnosis: What Each Type Can Mimic
Acute gout can resemble:
- Septic arthritis (a key emergency distinction)
- Cellulitis around a joint
- Pseudogout (CPPD crystal disease)
Chronic or tophaceous gout can resemble:
- Rheumatoid arthritis with nodules
- Psoriatic arthritis
- Osteoarthritis with inflammatory flares
- Soft tissue tumors or nodules
Crystal confirmation through aspiration is especially valuable in uncertain cases, and imaging can support diagnosis when aspiration is not feasible.
Treat-to-Target Urate Goals and Why They Matter
Effective long-term control depends on keeping urate low enough that crystals dissolve. The concept is simple: urate above saturation promotes deposition; urate below saturation promotes dissolution. Sustained control reduces flares, shrinks tophi, and slows joint damage.
The more advanced the disease, the more important consistent control becomes. In chronic and tophaceous gout, the goal is not just fewer flares; it is reducing total crystal burden.
Practical Self-Management by Gout Type
During Acute Flares
- Start prescribed anti-inflammatory therapy early
- Rest and elevate the affected limb
- Hydrate steadily and avoid alcohol binges
- Avoid sudden fasting or crash dieting
Between Flares (Intercritical and Chronic)
- Keep lifestyle consistent: hydration, weight management, balanced diet
- Review medications that may raise urate where clinically appropriate
- Track triggers, flare frequency, and urate levels
- Adhere to urate-lowering therapy if prescribed, even when symptom-free
With Tophi
- Monitor nodules for skin breakdown, drainage, or pressure pain
- Prioritize consistent urate control to shrink deposits
- Address footwear and joint support to reduce mechanical stress
- Seek evaluation for nerve symptoms, tendon pain, or functional limitations
Summary
Acute gout is about controlling sudden inflammation fast and recognizing triggers.
Chronic gout is about preventing frequent attacks and stopping ongoing joint inflammation by reducing urate consistently.
Tophaceous gout signals advanced crystal burden and requires aggressive, sustained urate control to dissolve deposits and prevent disability.
When urate is managed long-term, gout can move “backward” along this spectrum, with fewer flares, improved mobility, and shrinking tophi.