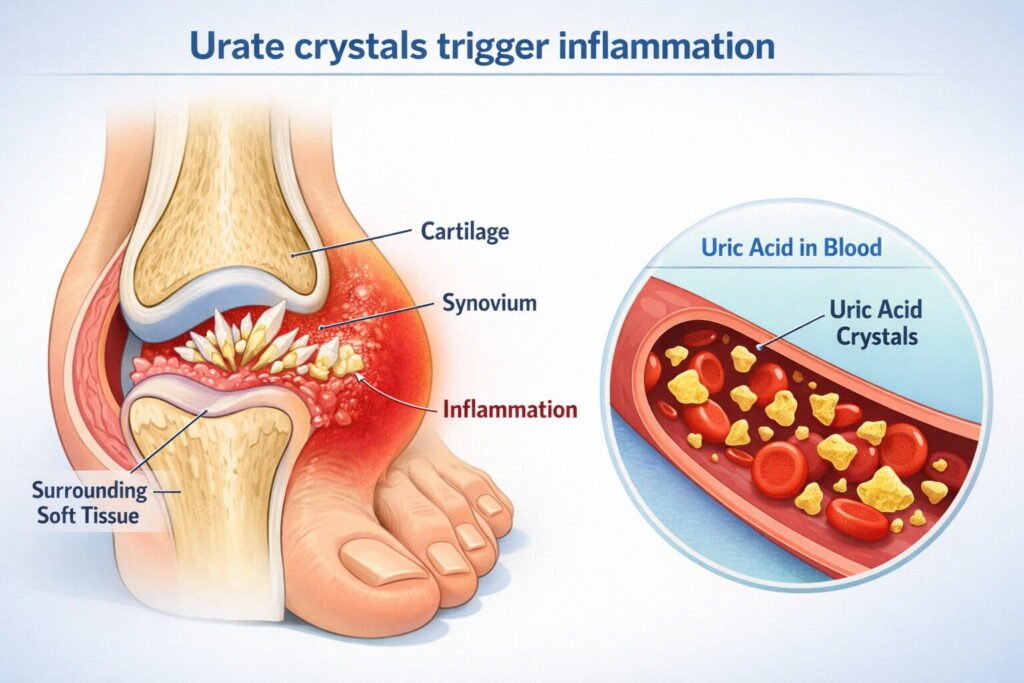
Gout is an inflammatory arthritis caused by monosodium urate crystal deposition in joints and surrounding tissues when blood uric acid stays high enough for crystals to form. If you are searching what is gout, this guide explains how gout develops, what a flare feels like, which tests actually confirm it, and how to choose treatment that fits your kidneys, stomach, heart, and daily life. It is written for mixed experience levels, from first time flares to recurrent attacks and complex cases with kidney disease or multiple medications. You will leave with a clear plan for flare control, urate lowering therapy, and long term risk reduction without confusing one for the other.
The biology of gout and why it happens now, not just later
Crystal formation depends on urate saturation, which is influenced by genetics, kidney clearance, hydration, body temperature, and sudden metabolic shifts that change urate levels quickly. Many people carry higher uric acid for years and then flare when a trigger causes a rapid rise or fall in urate, because changing levels can disturb existing deposits and activate immune cells. The immune response is driven by neutrophils and inflammatory signaling, which is why gout pain can feel explosive and why swelling can look dramatic compared with the size of the joint. Understanding that gout is both a metabolic condition and an immune mediated flare process helps you treat the attack now while preventing the next one with steady urate control.
• Think of a flare as an immune reaction to crystals, not a simple overuse injury.
• High uric acid increases risk, but a single lab result does not prove gout by itself.
• Cooler areas like toes can crystalize more easily because temperature affects solubility.
• Rapid urate change can trigger attacks even when overall urate is improving.
• Long term control requires keeping urate low enough for deposits to shrink over time.
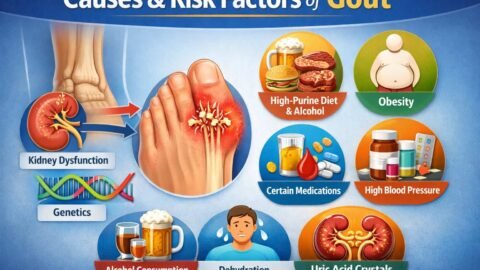
Causes and risk factors you can actually influence
Genetics strongly influences urate handling through transport proteins in the kidneys and gut, which is why gout often runs in families even when diets look similar. Kidney function matters because most urate leaves the body through the kidneys, so chronic kidney disease can raise urate and also limits certain medication choices. Lifestyle factors like higher body fat, frequent alcohol intake, dehydration, and sleep disruption can raise urate or increase flare likelihood by shifting hormones and kidney perfusion. Medications also play a major role, including certain diuretics and immunosuppressants, so gout prevention often starts with a careful medication review rather than only food changes.
• Ask your clinician whether any diuretic, low dose aspirin, or transplant medication could be contributing.
• Prioritize hydration on travel days, after workouts, and during heat exposure to reduce urate concentration.
• Limit binge alcohol patterns because sudden spikes and dehydration can provoke flares.
• If weight loss is a goal, avoid crash dieting because rapid breakdown of tissue can increase urate temporarily.
• Track flare timing around illness, fasting, and high stress periods because immune shifts can amplify attacks.
• Address sleep apnea if present because oxygen dips and metabolic stress can worsen urate handling.
Symptoms and how gout differs from lookalikes
Classic gout causes sudden severe pain, warmth, redness, and swelling, often starting at night and peaking fast, with the big toe joint being a common first site but not the only one. The skin can appear shiny and tense, and even a bedsheet can feel intolerable due to allodynia from intense local inflammation. Gout can also involve the midfoot, ankle, knee, wrist, fingers, and elbow, and later may present as more frequent attacks with shorter breaks between them. The tricky part is that gout can mimic infection, trauma, calcium crystal arthritis, and inflammatory arthritis, so pattern recognition must be paired with smart testing when the stakes are high.
- Gout flares often peak quickly and feel disproportionately painful compared with a simple sprain.
- Infection is more likely when there is fever, chills, rapidly spreading redness, or severe illness feeling.
- Calcium crystal arthritis can look similar but often targets larger joints in older adults.
- Rheumatoid arthritis usually causes persistent multi joint symptoms rather than sudden single joint attacks.
- Cellulitis can surround a joint but typically has more diffuse skin involvement than joint centered swelling.
- Tendon problems hurt with movement patterns, while gout pain can be constant even at rest.
Tests that confirm gout and when you need them most
Joint aspiration with crystal analysis is the most direct confirmation because it can show needle shaped negatively birefringent crystals, and it can also rule out joint infection, which is a medical priority. Blood uric acid is helpful for long term management but can be normal during a flare, so it should not be the only deciding factor when symptoms are severe or atypical. Ultrasound can detect signs like a crystal coating on cartilage and soft tissue changes, while dual energy CT can identify urate deposits in certain settings, especially when aspiration is not possible. The decision to test depends on how typical the presentation is, whether infection is plausible, whether more than one diagnosis could be present, and whether the result will change treatment safely.
When to suspect infection and why the next steps change
Any hot swollen joint with systemic symptoms must be treated as a possible infection until proven otherwise, because delayed antibiotics in true septic arthritis can permanently damage cartilage. Risk rises with recent skin breaks, immune suppression, prosthetic joints, poorly controlled diabetes, and recent joint injections, but infection can still happen without obvious risk factors. The key difference is that infection requires urgent evaluation and often joint aspiration, blood work, and sometimes imaging, while gout flare care alone is not enough if bacteria are present. If infection is on the table, avoid masking the picture with leftover antibiotics or repeated steroid dosing without evaluation, because you need a clear diagnosis to protect the joint and the person.
• Fever, rigors, or feeling acutely unwell should push you toward urgent evaluation.
• Rapidly increasing redness beyond the joint can suggest spreading skin infection.
• New severe pain in a prosthetic joint is an emergency until proven otherwise.
• Immune suppression increases the chance that infection looks less dramatic early on.
• Aspiration helps distinguish crystals from bacteria and guides safe treatment choices.
Table 1: Choosing the right test for your situation
| Test option | When to use | What it confirms | Common pitfalls | Safety notes | Who it fits best |
|---|---|---|---|---|---|
| Joint aspiration and fluid analysis | First episode, atypical joint, severe swelling, infection concern | Crystals and or bacteria | Not done when needed, sample delays | Small bleeding risk, sterile technique essential | Anyone with diagnostic uncertainty or red flags |
| Serum uric acid | Baseline planning and follow up once stable | Helps manage urate target strategy | Normal during flare, over interpreted | None beyond blood draw | People starting or adjusting urate lowering therapy |
| Ultrasound | When aspiration is hard or recurrence needs confirmation | Crystal signs and inflammation patterns | Operator dependent, early disease may be subtle | No radiation | Clinics with experienced musculoskeletal imaging |
| Dual energy CT | Complex cases, deep deposits, unclear diagnosis | Urate deposit mapping | Cost and availability, false positives from artifacts | Radiation exposure considerations | Refractory or atypical gout, surgical planning |
Treatment during a flare, fast relief without unsafe shortcuts
Acute treatment aims to shut down inflammation quickly using anti inflammatory medications that match the person’s kidney function, stomach risk, bleeding risk, and other medications. Nonsteroidal anti inflammatory drugs work well for many but can raise blood pressure, worsen kidney function, and irritate the stomach, so they are not a universal option. Colchicine can be effective when taken early, yet dosing must be adjusted for kidney disease and interactions, especially with certain antibiotics and antifungals. Corticosteroids, either oral or injected into a joint, can be highly effective and often safest for people who cannot take other agents, but repeated courses require a plan to prevent rebound flares and side effects.
• Treat early because the inflammatory cascade becomes harder to interrupt after the first day.
• Match drug choice to kidney function, ulcer history, blood thinners, and uncontrolled diabetes risk.
• Consider a single joint injection when one joint is involved and infection is ruled out.
• Use ice packs and elevation as add ons, not replacements, to reduce local inflammatory swelling.
• Avoid starting random leftover antibiotics because it complicates diagnosis if infection is possible.
• Do not rely on opioid pain medicines as primary treatment because they do not reduce inflammation.
Table 2: Flare medication options and safety fit
| Option | When it can help | What it does | Common pitfalls | Safety notes | Who it fits best |
|---|---|---|---|---|---|
| NSAIDs | Early flare with low kidney and GI risk | Reduces inflammatory prostaglandins | Too long duration, inadequate stomach protection | Kidney injury, ulcers, blood pressure effects | Younger or low risk adults without kidney disease or ulcers |
| Colchicine | Best within early hours, recurrent flares | Limits neutrophil activity | Overdosing, interactions | Dose adjust in kidney disease, watch interactions | People who can treat early and have reviewed meds |
| Oral steroids | Moderate to severe flare, multiple joints | Broad anti inflammatory effect | Too short taper, rebound | Blood sugar rise, mood changes, fluid retention | People with kidney disease or NSAID intolerance |
| Intra articular steroid | Single joint flare after infection ruled out | Local anti inflammatory relief | Injecting without ruling out infection | Requires sterile technique | Isolated joint involvement with accessible joint |
Urate lowering therapy, how it differs from flare treatment and why flares can increase at first
Long term gout control depends on lowering urate enough to dissolve existing deposits, which is why urate lowering therapy targets the root cause rather than the short term inflammation. The most commonly used agents reduce urate production or increase urate removal, and the right choice depends on kidney function, prior reactions, cardiovascular history, and other medications. A key concept is that starting urate lowering therapy can temporarily increase flares because changing urate levels mobilizes deposits and exposes crystals to the immune system, even though the long term trend is improvement. That is why flare prophylaxis is often prescribed when starting or increasing urate lowering therapy, using low dose anti inflammatory medication for a defined period based on clinical risk.
• Do not judge urate lowering therapy by the first few weeks because early flares can be part of the process.
• Aim for a steady urate level over time because stability helps deposits shrink gradually.
• Use prophylaxis so you can stay on the long term plan rather than stopping and restarting.
• Review kidney labs and interacting drugs before choosing the urate lowering medication.
• Discuss a target urate strategy with your clinician rather than focusing only on symptom relief.
Step by step: How to start a long term gout plan safely
A durable plan combines medication, monitoring, and trigger management while keeping infection risk and drug safety in view. Each step below is designed to reduce flares now and lower urate enough to prevent future damage over months, not days. The sequence matters because starting long term therapy without a flare plan is a common reason people quit early. Use this as a structured conversation guide for urgent care, primary care, or specialty visits.
- Confirm the diagnosis when uncertainty exists, especially for first episodes or unusual joints, and prioritize ruling out infection if red flags are present.
- Treat the current flare promptly with a medication choice tailored to kidney function, ulcer risk, blood thinners, diabetes control, and pregnancy considerations.
- Schedule a follow up visit after the flare settles to check uric acid, kidney function, liver enzymes if relevant, and medication interactions.
- Decide whether urate lowering therapy is indicated based on recurrence, tophi, kidney stones, chronic kidney disease, and joint damage pattern.
- Start urate lowering therapy at a conservative dose and increase gradually to reach a target urate strategy while minimizing rapid swings.
- Add flare prophylaxis for the first months of urate lowering therapy and set clear rules for what to do if a flare breaks through.
- Recheck labs at planned intervals, adjust doses based on urate and tolerability, and keep the long term medication consistent.
- Build a trigger reduction routine focused on hydration, alcohol pattern changes, weight trajectory, sleep quality, and medication review rather than extreme restriction.
Lifestyle and nutrition, realistic risk reduction without food myths
Diet influences urate, but in many people it is a smaller lever than genetics, kidney clearance, and medication effects, so the goal is smart risk reduction rather than perfection. Purine rich foods can raise urate, yet the pattern that matters most is repeated high load intake combined with dehydration or alcohol, which concentrates urate and stresses kidney excretion. Sugary drinks and high fructose patterns can increase urate production in the liver, while a balanced eating pattern with adequate fiber and lean proteins can support weight goals and metabolic health. Hydration, gradual weight change, and consistent routines help because urate handling is sensitive to sudden metabolic shifts, especially fasting, crash diets, or intense short term detox style regimens.
• Choose water as the default beverage, especially with travel, heat, or exercise.
• Keep alcohol as occasional and moderate, and avoid binge patterns that combine dehydration with urate spikes.
• Reduce sugary drinks and frequent high fructose snacks to lower urate production pressure.
• Favor steady weight loss if needed, because rapid loss can temporarily increase urate and provoke flares.
• Use balanced protein choices and keep portion sizes consistent rather than swinging between extremes.
• Track personal triggers in a simple log because individual sensitivity varies widely.
Table 3: Common trigger patterns and safer swaps
| Pattern | Why it can trigger gout | Safer swap | Common pitfalls | Who it helps most |
|---|---|---|---|---|
| Dehydration from heat, travel, or illness | Concentrates urate and reduces kidney clearance | Scheduled water intake and electrolytes when appropriate | Over correcting with sugary sports drinks | People with seasonal flares or frequent travel |
| Binge alcohol episodes | Raises urate and causes dehydration | Lower frequency and pairing with water and food | Assuming all alcohol is equal for every person | Social drinkers with weekend flare pattern |
| Crash dieting or prolonged fasting | Rapid metabolic shifts increase urate | Gradual calorie deficit with protein and fiber | Rapid loss followed by rebound eating | People targeting weight change |
| High sugar beverage routine | Increases urate production | Unsweetened drinks and whole food snacks | Switching to sweetened juices | People with metabolic syndrome features |
Special populations and medication safety decision points
Kidney disease changes gout management because reduced clearance increases urate while also limiting or modifying common flare drugs, making dosing and monitoring essential rather than optional. Blood thinners increase bleeding risk for certain pain medicines and raise the stakes for avoiding stomach irritation, so medication selection must be individualized. Diabetes can complicate steroid use because blood sugar can rise quickly during a course, which calls for a plan for glucose checks and short term adjustments. Pregnancy and breastfeeding require extra caution, and anyone who is pregnant or trying to conceive should make medication decisions with a clinician who can match benefits and risks carefully.
• In chronic kidney disease, avoid self dosing flare medicines without dose guidance because accumulation can be dangerous.
• If you take anticoagulants, prioritize options that minimize GI bleeding risk and check for drug interactions.
• With diabetes, plan for blood glucose monitoring when steroids are used and discuss temporary medication changes.
• For pregnancy or breastfeeding, treat gout as a medical decision, not a supplement project, because safety profiles vary.
• If you have a transplant or immune suppression, lower the threshold for infection evaluation and aspiration.
• If you have recurrent kidney stones, discuss urine evaluation and stone prevention strategies alongside urate control.
Two realistic scenarios that show how decisions change
A 38 year old software engineer in the UK develops sudden right big toe pain after a weekend with heavy takeaway meals, alcohol, and a long flight, and the toe is red, hot, and exquisitely tender without fever; the pattern is typical, so the urgent goal is rapid anti inflammatory treatment and a follow up plan, not imaging for everything at once. He has no kidney disease and no ulcer history, so an NSAID course or early colchicine could be reasonable, combined with hydration and avoiding repeating the trigger pattern while scheduling labs after the flare resolves. Because this is a first episode, he and his clinician discuss whether confirmation is needed now versus watchful follow up, and they decide to plan a definitive diagnosis if another flare occurs or if the pattern becomes atypical. The long term win is not a strict food ban, but a consistent routine that avoids dehydration and binge triggers, and a clear rule for early flare treatment so the next attack is shorter and less disruptive.
A 72 year old retiree in the US with chronic kidney disease, atrial fibrillation on anticoagulation, and type 2 diabetes develops a swollen warm left knee with severe pain and mild malaise after a recent skin tear on the lower leg; her risk profile raises concern for infection even if she has a history of gout. Because the knee is large and new symptoms include feeling unwell, she needs urgent evaluation with joint aspiration to check for bacteria and crystals, since the management pathways are completely different. While waiting for results, medication choices are conservative due to kidney function and bleeding risk, and if infection is ruled out, a carefully planned steroid strategy or joint injection may be safer than NSAIDs, with glucose monitoring support. Once stabilized, she benefits from a structured urate lowering therapy plan with prophylaxis and close lab follow up, because recurrent knee flares in a high risk patient can lead to functional decline and repeated urgent visits.
Common mistakes and fixes that prevent repeat flares
Many people treat the pain but skip the long term urate plan, which allows crystals to persist and makes the next flare more likely, so the fix is to pair flare treatment with a follow up appointment to discuss urate lowering therapy when indicated. Another common error is stopping urate lowering therapy during a flare, which can destabilize urate and prolong the cycle, so the fix is to continue long term therapy unless a clinician tells you to stop for safety reasons. People also over rely on a single uric acid test taken during the flare, which can mislead decisions, so the fix is to recheck once stable and use a trend with context. Finally, ignoring infection red flags can be dangerous, so the fix is to treat any fever, systemic illness, prosthetic joint pain, or unusual presentation as urgent until proven otherwise.
• Mistake: Waiting several days before treating a flare, Fix: keep a prescribed plan at home and treat at the first clear signs.
• Mistake: Using leftover medicines with the wrong dose, Fix: confirm dosing for your kidney function and interacting drugs.
• Mistake: Extreme diet restriction followed by rebound eating, Fix: use steady routine changes that you can repeat weekly.
• Mistake: Assuming gout cannot occur with normal uric acid during an attack, Fix: use clinical pattern plus appropriate confirmation.
• Mistake: Skipping prophylaxis when starting urate lowering therapy, Fix: ask for a prevention bridge so you stay consistent.
• Mistake: Treating a potentially infected joint as gout at home, Fix: seek urgent care when red flags appear.
Pro tips and edge cases that clinicians watch for
Tophi are firm deposits that can appear on ears, fingers, elbows, or around joints, and their presence usually signals a higher crystal burden that benefits from sustained urate lowering therapy with close monitoring. Some people present with gout in unusual sites like the spine, tendon sheaths, or small hand joints, which can mimic nerve compression or inflammatory arthritis and may require advanced imaging or aspiration. Early in urate lowering therapy, breakthrough flares are not a failure, and the pro move is to treat the flare while maintaining the long term dose plan, because stopping and restarting can create more volatility. Another edge case is when multiple conditions coexist, such as gout plus calcium crystal arthritis or gout plus osteoarthritis, where pain can have more than one driver and treatment may need layered strategies.
• If flares become more frequent or move to multiple joints, ask about tophi assessment and long term urate goals.
• If symptoms persist between attacks, consider joint damage or overlapping arthritis rather than assuming constant gout.
• If you have repeated ankle or midfoot flares, check footwear and gait stress because local trauma can amplify inflammation.
• If you start a new medication and flares appear, request a medication review rather than blaming only food.
• If you have kidney stones, discuss urine chemistry and hydration targets because stone prevention may need specific steps.
Quick Checklist
• Identify whether the pattern is typical gout or if infection could be present based on fever, systemic illness, or prosthetic joint pain.
• Treat the flare early with a medication choice that fits kidney function, stomach risk, blood thinners, and diabetes control.
• Use hydration, elevation, and ice as supportive measures without delaying anti inflammatory treatment.
• Plan follow up labs after the flare settles to guide long term urate decisions and medication safety.
• If urate lowering therapy is started, use prophylaxis and keep dosing steady rather than stopping during flares.
• Track personal triggers like dehydration, binge alcohol, fasting, illness, and medication changes to reduce recurrence.
If You Only Do 3 Things
• Get urgent evaluation for any hot swollen joint with fever, severe illness feeling, prosthetic joint, or high infection risk factors.
• Separate flare treatment from long term urate lowering therapy, and use prophylaxis when starting or increasing urate lowering medication.
• Build a repeatable routine around hydration, stable weight trajectory, and medication review to reduce urate swings.
FAQs
Can gout happen with a normal uric acid test during an attack?
Yes, uric acid can be lower or normal during a flare because inflammation and shifting fluid balance can change measured levels, and crystals can still be present in the joint. The most reliable confirmation is crystal identification in joint fluid, with imaging sometimes supporting the diagnosis when aspiration is not feasible. If your result was normal during an attack, rechecking after symptoms settle is often more useful for long term planning. Decisions should consider the whole clinical picture, not a single number.
What is the fastest way to calm a gout flare?
Fastest relief usually comes from early anti inflammatory treatment matched to your health profile, such as an appropriate NSAID, correctly dosed colchicine, or corticosteroids. Time matters because inflammatory signaling escalates quickly, so delays often lead to longer pain duration. Supportive steps like ice and elevation help but rarely replace medication when inflammation is intense. If infection is possible, urgent assessment is the priority before escalating steroids.
Should I stop urate lowering therapy when I have a flare?
In most cases you continue long term urate lowering therapy during a flare, because stopping can destabilize urate and prolong the overall cycle. The flare is treated with anti inflammatory medication while the urate plan stays consistent. The exception is if a clinician advises stopping for a specific safety reason, such as a serious reaction. If you are unsure, contact your prescriber rather than making a sudden change.
Why can starting urate lowering therapy trigger more flares at first?
When urate levels start to fall, old deposits can begin to break up and expose crystals to the immune system, which can provoke attacks even though you are moving in the right direction. This is why prophylaxis is used during the early phase, often with low dose anti inflammatory medication for a period based on risk. Over time, steady low urate reduces crystal burden and flares usually become less frequent. The goal is consistency through the early bump.
Is gout only caused by diet?
No, diet is only one contributor, and genetics plus kidney clearance often play a larger role. Medications, body composition, hydration status, alcohol pattern, and comorbid conditions can all shift urate and flare risk. Diet changes can help, especially reducing sugary drinks and binge patterns, but they are not always sufficient alone. Many people need a medication based plan to reach sustained urate control.
What tests are most important for recurrent gout?
For recurrent cases, periodic uric acid checks after flares resolve help guide urate lowering therapy dosing, and kidney function monitoring supports safe medication choices. If diagnosis was never confirmed and symptoms are atypical, joint aspiration or advanced imaging may be appropriate. Imaging can also help assess deposit burden in complex cases. The best test set is the one that changes management safely, not the one that is most available.
How does kidney disease change gout treatment?
Kidney disease can raise urate by reducing clearance and can also limit the safe use or dosing of common flare drugs, especially NSAIDs and colchicine. Steroids or carefully planned local injections may be preferred in some situations, and urate lowering therapy choices and dosing may differ. Monitoring becomes more important because medication accumulation and side effects can occur more easily. A kidney aware plan reduces both flares and complications.
Can gout affect more than the toe?
Yes, gout often starts in the toe but can involve ankles, knees, midfoot, wrists, fingers, and elbows, and sometimes presents in less typical areas in advanced disease. Recurrent inflammation can contribute to joint damage and functional limits over time. Tophi can develop in soft tissues and are a sign of higher crystal burden. Long term urate control helps prevent progression beyond the first joint.
Is joint aspiration painful and is it worth it?
Joint aspiration can be uncomfortable, but it is usually brief and can provide decisive information, especially when infection is a concern or the diagnosis is unclear. It can also relieve pressure in some swollen joints. The value is highest in first episodes, unusual joints, immunosuppressed patients, and anyone with fever or systemic symptoms. Knowing whether bacteria are present can protect the joint and guide urgent treatment.
Conclusion
Gout is a crystal driven inflammatory arthritis that can be treated effectively when you separate immediate flare control from long term urate reduction. The safest path is early targeted anti inflammatory treatment, rapid attention to infection red flags, and a steady urate lowering therapy plan with prophylaxis when indicated. Pair your medication strategy with repeatable routines that reduce dehydration and sudden urate swings, and use follow up labs to keep decisions grounded. If your flares are recurrent, severe, or complicated by kidney disease or blood thinners, bring a structured plan to your clinician so treatment stays effective and safe.
Sources
[1] Centers for Disease Control and Prevention: Public health guidance and patient education
[2] National Health Service: Patient information and clinical care pathways
[3] World Health Organization: Global health context and chronic disease frameworks
[4] American College of Rheumatology: Specialty guidance for gout management
[5] British Society for Rheumatology: Rheumatology standards and clinical recommendations
[6] Kidney Disease Improving Global Outcomes: Nephrology guidance relevant to urate and kidney disease
[7] National Institute for Health and Care Excellence: Evidence based guideline development
[8] Cochrane: Systematic reviews and evidence synthesis
[9] U S Food and Drug Administration: Medication safety communications and prescribing information standards
[10] American College of Radiology: Imaging appropriateness and radiology standards